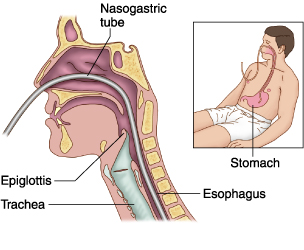
Nasogastric tube insertion is a medical procedure that involves inserting a nasogastric tube through the nose, throat and goes down to the stomach.
Why do we use NG tube insertion?
- Inserting a nasogastric tube enables you to drain gastric contents, decompress the stomach and introduce a passage into the GI tract.
- It allows treating gastric immobility and bowel obstruction.
- Nasogastric tube insertion also allows drainage or lavage in drug overdose or poisoning. Nasogastric tube insertion is used in trauma settings.
- NG tubes are used to prevent vomiting and aspiration, and it can be also used for assessment of GI bleeding.
- Nasogastric tube insertion can be used for enteral feeding initially.
<< back to Medical Nursing Videos
What Is Nasogastric NG Tube Insertion Video
Videos on
this site are for demonstration purposes only. Please
do not attempt any of the procedures seen in these videos
without formal medical education & licensing.
Nasogastric tube insertion contraindications:
The only contraindication for nasogastric tube insertion is when there is a presence of severe facial trauma. In this case an orogastric tube may be inserted.
 What Is Nasogastric Tube Insertion Complications?
What Is Nasogastric Tube Insertion Complications?
There are two main complications of NG tube insertion, aspiration and tissue trauma. The placement of the catheter can cause gagging or vomiting, for that matter suction should always be ready to use in case like this.
Precautions:
NG tube insertion requires an experienced operator. Gloves must be worn while starting an NG; the risk of vomiting is high and the operator’s face and eyes must be protected. All team members as well as the operator must wear gloves, face, eye protection and gowns.
NG tube insertion Equipment:
Before this procedure starts all the necessary equipment should be prepared and available at the bedside prior. This equipment includes:
- Personal protective equipment
- Nasogastric or orogastric tube
- Catheter tip irrigation 60ml syringe
- Water-soluble lubricant, 2% Xylocaine jelly
- Adhesive tape
- Low powered suction device OR Drainage bag
- Stethoscope
- Ice chips
- Emesis basin
- pH indicator strips
Introduction of the NG tube insertion:
Before you start the NG tube insertion you should give your patient reassuring and detailed explanation about the procedure, explain the reasons and why this tube is necessary.
Nasogastric tube sizes:
The nasogastric tubes come in various sizes like: 8, 10,12,14,16 and 18Fr. The easiest tubes for insertion are the stiff tubes. If there are in a refrigerator of filled with saline they become even stiffer. Sometimes there are some fine-bore tubes that come with a guide to aid placement. All the tubes have markings and a radio-opaque marker at the tip to check its position on X-ray.
What Is The NG tube insertion preparation?
The preparation for this procedure starts with washing hands. After washing hands the practitioner has to prepare a trolley that includes: gloves, local anesthetic jelly or spray, 60ml syringe, pH strip, kidney tray, sticky tape and a bag. The bag is used to collect secretions.
NG tube insertion process!
NG tube is usually inserted by a nurse or junior doctor by the bedside or in theatre by a anesthetist before or during surgery. An external measurement is taken from the tip of the nose to a point halfway between the xiphoid and the umbilicus distance. This measurement gives a rough idea of the required length.
The tube is chosen and the tip is lubricated by smearing aqua gel or local gel. The practitioner is going to choose the eider nostril and tube id going to slid down along the floor of the nasal cavity. We have to give our patient to drink a small amount of water; it is going to help to direct the tube into the oesophagus as well as release our patient’s gagging. Once the tube is in the oesophagus it is a lot easier to push it down into the stomach. The correct intragastric position is verified (below this text you can see the verification).
The tube is fixed to the nose and forehead with adhesive tapes. The stomach is going to be decompressed by attaching a 60ml syringe. The blocked tubes can be flushed open with saline or air.
Verification of the correct intragastric position
There are two ways to confirm the tube’s position: pH test and X-ray.
pH test- the tube is aspirated and the contents are checked using pH paper. If you take a proton pump inhibitor or H2 receptor antagonist it may alter the pH. Intake of milk can neutralize the acid.
Chest X-ray- The practitioners use X-ray to check the tube’s location. X-ray is used for patients who have swallowing problems, confused patients and for those in ICU. For these kinds of situations a chest X-ray must be taken including the upper half of the abdomen.